In the years before the historic Roe v. Wade decision, women in the United States seeking an abortion faced a perilous path. Safe options for abortion were limited and unsafe procedures resulted in high maternal mortality rates. The tide started to turn in the 1960s, when some states began expanding the circumstances under which abortion was legal, and when a group of women started the Jane Collective, an underground system that helped women find safe and affordable abortions outside of the formal legal and health systems.
In 1973, the Roe v. Wade Supreme Court decision determined that abortion was legal—recognizing not only that laws prohibiting abortion violated a woman’s constitutional right to privacy, but also that forcing women to seek medical care that had been deemed illegal caused an unnecessary burden on women and on the health care system.
In the 45 years that abortion has been legal in the United States, it has been established as an extremely safe medical procedure. A recent report showed that complications with abortion care are rare: less frequent than complications with wisdom teeth extraction and tonsillectomies, for example.[i] In contrast, the accessibility of the service—which includes availability and affordability—has steadily declined. Over a thousand abortion restrictions have been enacted in states across the country.[ii] Unnecessary and burdensome restrictions such as physician and hospital requirements, mandated parental involvement for minors, and allowing providers to refuse to provide the service have caused clinics to close, limited the availability of abortion services, and forced many women to travel great distances to receive care.
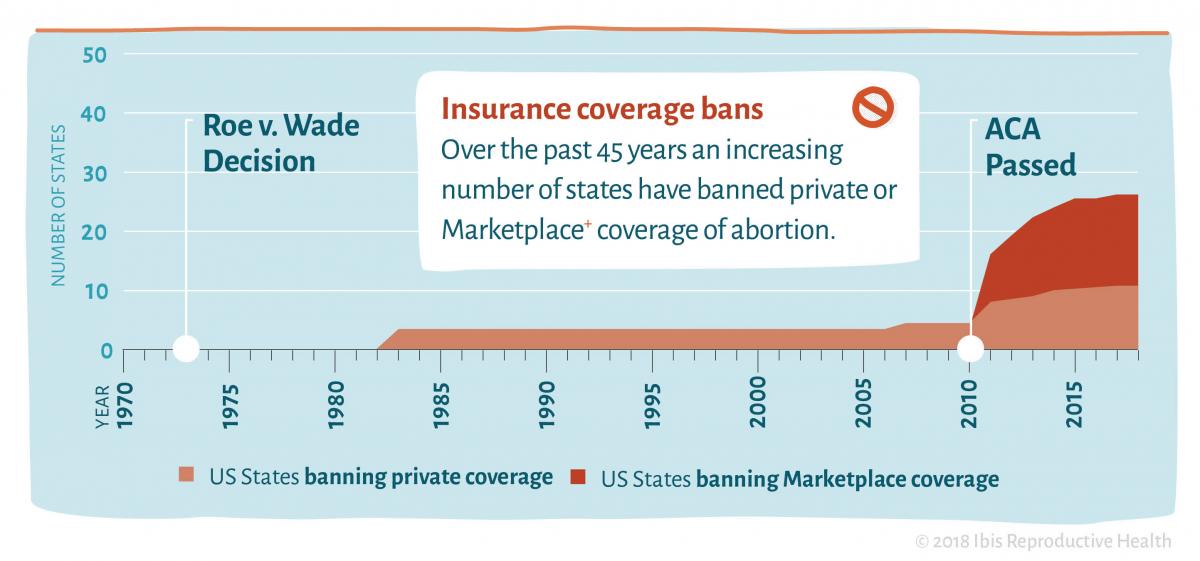
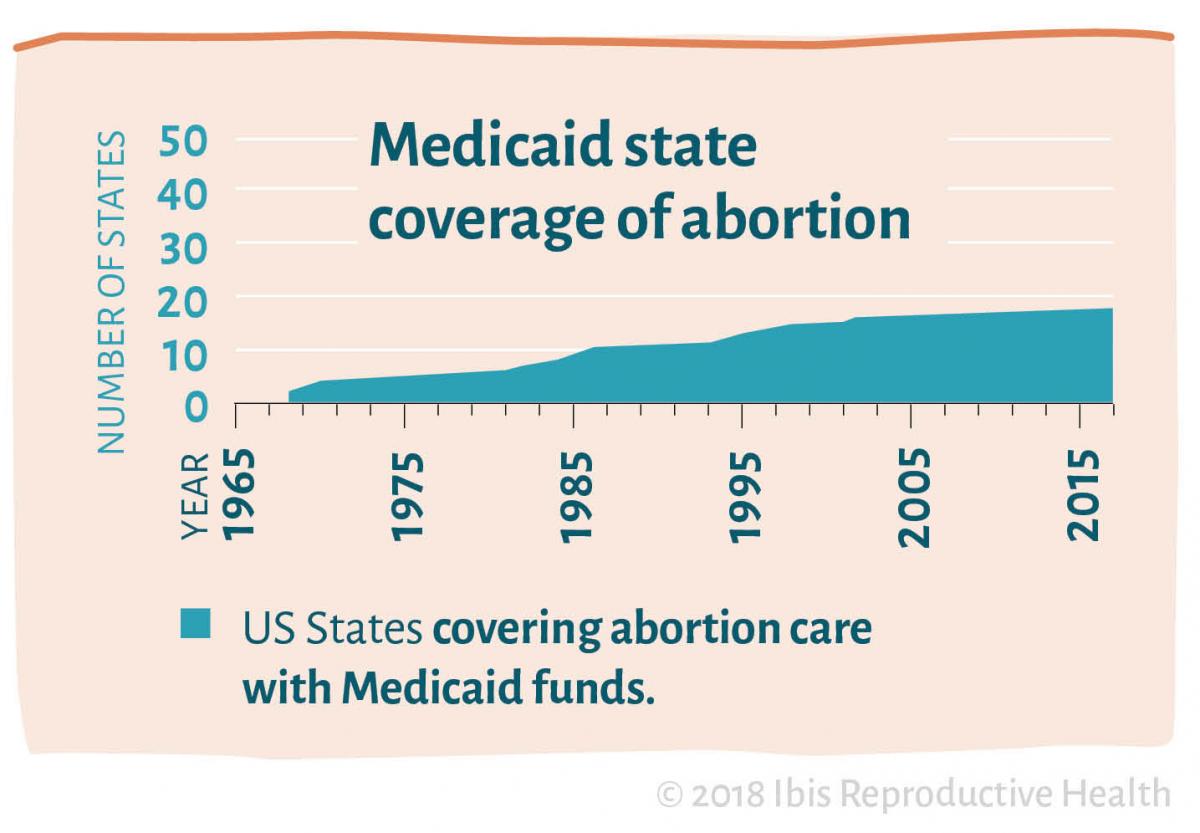
In addition to the restrictions on clinics and providers, lawmakers in many states have severely limited the affordability of abortion. In the years after Roe v. Wade, Congress passed the Hyde Amendment, preventing the use of federal Medicaid funds to cover abortion services and forcing many women with Medicaid to pay for the costs of an abortion out-of-pocket.[iii] Thirty-four states (including Washington, DC) follow the restrictions imposed by the Hyde Amendment, while 17 have laws that allow for state Medicaid funds to cover abortion.[iv] Following this Amendment, Congress passed additional restrictions on abortion care for women who are covered under other public health care programs, including military service members and their families, those seeking services from the Indian Health Services, and Peace Corps Volunteers, among others. In recent years, the influence of the Hyde Amendment has grown, with many individual states also restricting private insurance coverage of abortion.[v][vi] **
Restrictions on abortion coverage and availability render the legal ruling of Roe v. Wade a right that only some can actualize and place women in the dangerous position of having to find alternatives to a safe and legal health procedure. About 7.4 million women aged 15-49 who have health insurance through Medicaid live in states where they cannot use their insurance to cover abortion in most circumstances.[vii] Most significantly impacted are low-income women, who are often either unable to pay the out-of-pocket cost for abortion care, or are unable find the funding in a timely manner.[viii] Our research has found that women who have Medicaid and have to pay for an abortion out-of-pocket have to make sacrifices to afford the procedure, including foregoing rent and groceries. Some women find the costs so prohibitive that they choose to continue the pregnancy.
The promise of Roe is a nation where women have the legal right and access to the health care they need—but there is much still to be done to make that right a reality. Though many states have been acting to further restrict abortion coverage (and the Trump administration is considering further limiting availability by empowering the office in charge of civil rights at the Department of Health and Human Services to protect health workers who have moral objections to performing abortions), there are others who are working to realize the promise of Roe for all women. States such as California, New York, Oregon, and Illinois have taken steps to protect a woman’s right to abortion care by implementing laws that mandate insurance coverage of abortion care[ix],[x],[xi],[xii].
We strive for a country where punitive barriers are eliminated and where all women have equal access to sexual and reproductive health services, including abortion. We urge you to join this fight by supporting coalitions that work to dismantle barriers to abortion access and ensure that all people—regardless of income—can receive the care they need.
---------------------------------------------------------------------------------------------------------------
[i] Safety of abortion in the United States. Advancing New Standards in Reproductive Health, University of California San Francisco. Available from: https://www.ansirh.org/sites/default/files/publications/files/safetybrief12-14.pdf
[ii] E Nash et al., Policy trends in the states: 2017. Guttmacher Institute. 2018. Available from: https://www.guttmacher.org/article/2018/01/policy-trends-states-2017.
[iii] Salganicoff AR, C.; Sobel, L. The Hyde Amendment and Coverage for Abortion Services. Kaiser Family Foundation. 2016. Available from: http://www.kff.org/womens-health-policy/perspective/the-hyde-amendment-and-coverage-for-abortion-services/.
[iv] Salganicoff AR, C.; Sobel, L. The Hyde Amendment and Coverage for Abortion Services. Kaiser Family Foundation. 2016. Available from: http://www.kff.org/womens-health-policy/perspective/the-hyde-amendment-and-coverage-for-abortion-services/.
[v] Donovan MK. In real life: Federal restrictions on abortion coverage and the women they impact. Guttmacher Policy Review. January 5, 2017. Available at: https://www.guttmacher.org/gpr/2017/01/real-life-federal-restrictions-abortion-coverage-and-women-they-impact.
[vi] Salganicoff AS, Sobel L, Kurani N, Gomez, I. Coverage for abortion Services in Medicaid, marketplace plans and private plans. Kaiser Family Foundation. January 2016. Available at: http://www.kff.org/womens-health-policy/issue-brief/coverage-for-abortion-services-in-medicaid-marketplace-plans-and-private-plans/.
[vii] Salganicoff AS, Sobel L, Kurani N, Gomez, I. Coverage for abortion Services in Medicaid, marketplace plans and private plans. Kaiser Family Foundation. January 2016. Available at: http://www.kff.org/womens-health-policy/issue-brief/coverage-for-abortion-services-in-medicaid-marketplace-plans-and-private-plans/.
[viii] All Above All, Ibis Reprodudtive Health. Research brief: The impact of medicaid coverage restrictions on abortion. Ibis Reproductive Health. 2016. Available from: https://ibisreproductivehealth.org/publications/research-brief-impact-medicaid-coverage-restrictions-abortion.
[ix] Abortion Is Basic Health Care. ACLU of Northern CA. August 2014. Available from: https://www.aclunc.org/blog/abortion-basic-health-care.
[x] Press Release - Governor Cuomo Announces Decisive Actions to Secure Access to Reproductive Health Services in New York. New York Department of Financial Services. January 2017. Available from: http://dfs.ny.gov/about/press/pr1701211.htm.
[xi] Reproductive Health Equity Act. Oregon Health Authority: Reproductive and Sexual Health : State of Oregon. Available from: http://www.oregon.gov/oha/PH/HEALTHYPEOPLEFAMILIES/REPRODUCTIVESEXUALHEALTH/Pages/reproductive-health-equity-act.aspx.
[xii] Illinois General Assembly - Bill Status for HB0040. 100th General Assembly. September 2017. Available from: http://www.ilga.gov/legislation/billstatus.asp?DocNum=40&GAID=14&GA=100&DocTypeID=HB&LegID=99242&SessionID=91.